How pharmacists can use CGM data to end ‘clinical inertia’ in diabetes care

To mark Diabetes Awareness Week (8 June – 12 June), The Pharmacist spoke to Adam Dawes, senior medical affairs manager for Dexcom UK and Ireland, and Jo Lloyd, a diabetes nurse and medical educator for Abbott based in the Black Country, about how pharmacists can use continuous glucose monitoring (CGM) data to improve their diabetes consultations.
‘Continuous glucose monitoring has been around in various different guises since the 1960s and in the realm of the specialist for the past 25 years, but it is something that should be in the generalist toolkit too,’ says Adam Dawes, senior medical affairs manager at Dexcom UK and Ireland.
The development of continuous glucose monitors (CGM) has revolutionised the landscape of diabetes care and in March 2022, the National Institute for Health and Care Excellence (NICE) updated its type 1 diabetes guidelines to recommend that all adults with type 1 diabetes, about 350,000 people, should be offered a CGM. Some adults with type 2 diabetes may also be given access.
CGM can be offered by a patient's GP, diabetes specialist team or hospital diabetes clinic - depending on their integrated care board’s formulary. Each sensor lasts 10 to 15 days and they are issued on a standard NHS repeat prescription to be dispensed by community pharmacists.
For many years, it was the role of diabetologists, endocrinologists, and diabetes specialist nurses to interpret the data generated by these CGMs. But as access to the device has expanded, so too has the role of primary care clinicians in using CGM data to inform the care they offer.
What is a CGM?
A CGM has a thin, flexible filament coated in different kinds of electrodes, which is inserted under the skin using a small needle.
The sensor doesn’t sit directly in the bloodstream but reacts instead with glucose in the interstitial fluid – liquid found in the spaces between cells – and the electrical signal created by that reaction is then processed by the CGM and turned into a blood glucose reading. For most sensors, this takes place every five minutes (288 times a day) – and some sensors read as often as once per minute giving more than 1,000 readings a day.
Mr Dawes says: ‘CGM completely changed the game because it is continuous, so you have constant access to data which enables people to make better decisions. Not just healthcare professionals but people living with diabetes as well.’
Prior to the invention of CGMs, people with diabetes had to prick their finger multiple times a day to test their blood glucose – a process that was both cumbersome and provided limited information about how someone’s blood glucose levels were fluctuating.
Mr Dawes says managing diabetes this way is like driving home with your eyes closed and only being able to open them once every five minutes. ‘Do you think you’re going to get home OK? Wouldn’t it be easier if your eyes were open the whole time and you could see what was going on?’ he asks.
Finger prick testing is like driving home with your eyes closed and only being able to open them once every five minutes.
Ms Lloyd thinks having a CGM is about empowering individuals to manage their own health.
‘Think about the multiple decisions we make every day, then add to that the all the decisions someone with diabetes has to make. It is a challenge every single day, but CGMs support that decision-making,’ she says.
‘Diabetes distress’ or burnout is a well-documented product of this, affecting one in four people with type 1 diabetes and one in five people with type 2 diabetes, according to Diabetes UK.
Ms Lloyd says: ‘You don’t need in‑depth specialist knowledge to make a difference. For pharmacists, the crucial things to understand are the basics of the device and which patients are likely to benefit.’
How should pharmacists interpret CGM data?
According to Mr Dawes, there are two key things to look at in CGM data: ‘time in range’, and episodes of hypoglycaemia.
‘Time in range’ is the amount of time spent with a blood glucose between 3.9mmol/l and 10.0mmol/l, which is considered a healthy range. If a person’s CGM data shows that they are in range 70% of the time, their risk of future complications is significantly reduced, according to international consensus guidelines.
People with diabetes should also aim to spend less than 5% of their time with a blood sugar below 3.9mmol/l, or they run the risk of losing their ‘hypo awareness’ – meaning they stop being able to feel when their blood sugar is too low. For those who are older and frailer they should not be below 3.9mmol/l at all.
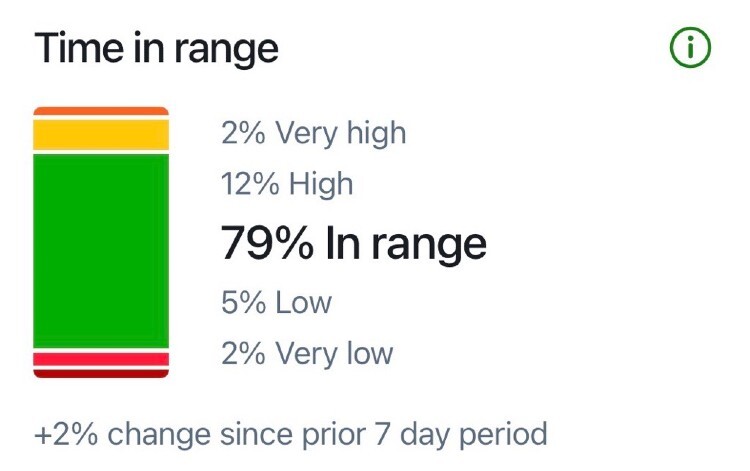
Picture 1: CGM data showing the percentage of time spent 'in range' or between 3.9mmol/l and 10.0mmol/l
Before CGM, a blood test every 3-6 months was the only way to measure how well someone was managing their diabetes.
Mr Dawes says: ‘Having access to CGM data helps primary care clinicians break the clinical inertia spiral, which happens during that three to six month period when you’re waiting for a diabetic person’s blood test results and there’s nothing else you can do.
‘CGM data allows pharmacists to have more informed discussions with people with diabetes, rather than just saying: “Your HBA1c is bad”. It’s about bringing together the data and the human touch; moving the conversation towards behaviour change and not just flooding people with numbers.’
Pharmacists may find CGM data particularly useful when speaking to patients with type 2 diabetes.
Mr Dawes says: ‘Managing type 2 diabetes is more complex, with a focus on managing someone’s whole health as opposed to just focusing on their glucose and I think this is where CGM data is going to help primary care clinicians and pharmacists.’
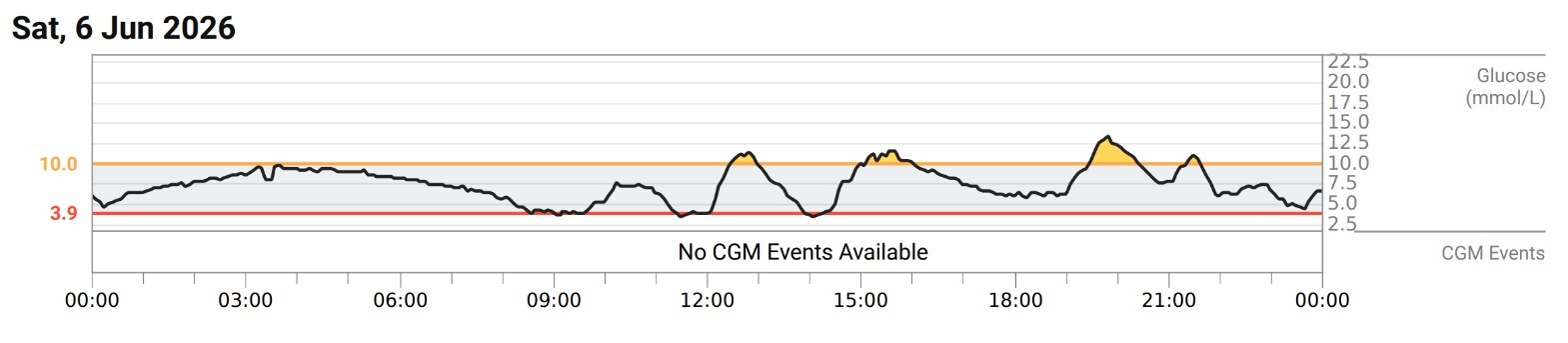
Picture 2: CGM data showing blood sugar levels during a 24-hour period
A recent study, funded by Abbott and and involving 303 participants across 24 clinical sites in the UK, found that people with type 2 diabetes using Abbott’s FreeStyle Libre CGM technology had better outcomes than those using traditional finger pricking.
At four months, participants using a Libre system for continuous glucose monitoring spent about 2.5 more hours a day in range demonstrating the benefit of real-time glucose information for people with type 2 diabetes.
Both Abbott and Dexcom offer CGM training for primary care clinicians, online and in-person. Abbot’s virtual learning hub is called ‘The Libre Academy’ and Dexcom’s equivalent, the ‘Dexcom Education Hub’, has a learning journey specifically for pharmacists.
Ms Lloyd says she has seen a growing number of pharmacists attending Abbott’s in-person CGM training because ‘pharmacists now see themselves as playing an important role in diabetes technology and are actively reaching out for that knowledge’.
What is the role of pharmacists in improving access to CGMs?
National Institute for Health and Care Excellence (NICE) guidelines say that everyone in England, Scotland and Wales with type 1 diabetes should be offered a CGM.
And CGM can also be considered for people with type 2 diabetes who:
- Use insulin two or more times a day; and
- Have recurrent or severe hypoglycaemia;
- Have impaired hypoglycaemia awareness;
- Can’t monitor their own blood sugar levels but could use a scanning device or have someone else scan for you; or
- Would otherwise be advised to do a finger prick test at least eight times a day.
However, access can differ depending on local policy and awareness – this is where pharmacists come in.
Ms Lloyd says: ‘There are still people with type 1 diabetes in the community who aren’t accessing CGM, particularly those in care settings or with certain vulnerabilities like learning disabilities.
‘In areas like Birmingham and the Black Country with high deprivation, digital literacy issues and many patients whose first language isn’t English, pharmacists are sometimes the only professionals who see those patients. That puts them in a key position to make sure people who are eligible for CGM aren’t missed.’
If pharmacists can identify who will benefit from the technology, they can actively advocate for those patients by speaking to their GP or diabetes specialist team, Ms Lloyd adds.
She describes a local primary care-led diabetes pilot – co-developed by a commissioning pharmacist and a diabetes nurse several years ago – which improved access to CGM and outcomes for people with diabetes in the area.
‘That early primary care network (PCN) pilot really changed people’s thinking. It proved that initiating CGM in primary care is both safe and effective, and it showed how pharmacists can work with specialist teams to widen access and reduce health inequalities,’ Ms Lloyd says.
Initiating CGM in primary care is both safe and effective, and pharmacists can work with specialist teams to widen access and reduce health inequalities.
In the UK, 5.8 million people are living with diabetes and, according to Diabetes UK, it estimated that diabetes will cost the NHS nearly £18bn by 2035 if prevalence continues to rise at the current rate.
The future of CGM
CGM data does not currently feed into patients’ primary care record, but Mr Dawes says Dexcom is looking to expand in this area, so it is a ‘definite possibility in the near future’.
Abbott also confirmed that it was looking at ways to integrate Libre data into NHS medical records, making it possible for pharmacists to access the same blood glucose data as specialist teams.
Ms Lloyd believes this would improve collaboration between primary and specialist care and prevent people with diabetes from having to attend multiple appointments.
The non-diabetes space is where Dexcom is heading next, according to Mr Dawes. ‘We’re the smartwatch generation – we are used to getting feedback on our health, how many steps we’ve done, how fast our heart rate is – so the next logical step is getting feedback on how our blood glucose reacts to different foods,’ he says.
‘Will Dexcom have a role in the prevention of diabetes in the future? That’s something we’d consider. Behaviour changes are a handy by product of having a CGM, so it could definitely have a role in managing prediabetes.’
Abbott is already working to combat prediabetes with a different sensor, Lingo, which helps people without diabetes to identify habits that keep their glucose in a healthy range more often.

Have your say
Please add your comment in the box below. You can include links, but HTML is not permitted. Please note that comments are not moderated before publication and the views expressed are those of the user and do not reflect the views of The Pharmacist. Remember that submission of comments is governed by our Terms and Conditions. You can also read our full guidelines on article comments here – but please be aware that you are legally liable for any libellous or offensive comments that you make. If you have a complaint about a comment or are concerned that a comment breaches our terms and conditions, please use the ‘Report this comment’ function to alert our web team.