
10:05am: Putting patient safety at the heart of organisational excellence

Chairing the forum, Janice Perkins
Chair for the day Janice Perkins, chair of the Pharmacy Voice Safety Group and pharmacy superintendent at Well, takes the stage.
We are quite clear there is no competitive advantage in driving the safety agenda.
We are a group of like-minded individuals and we are passionate about patient safety - 18 largest multiples plus the NPA.

Organisations signed up to safety
We are committed to making a difference and sharing our learning and experience.
We have five Sign up to Safety pledges:
1. Putting safety first
2. Continually learning
3. Being honest
4. Collaborating
5. Being supportive
We want to drive a safety culture that underpins pharmacy, it's about safety being part of the core things we do in pharmacies.
It should be the ingredients in a cake, not the icing that goes on top of it.
There's a lot of change in pharmacy: EPS, automation, hub-and-spoke, and through this we are going to champion safety. The key message is about reporting, sharing and learning.
We will be issuing a detailed work plan in the new year.
10:15am: Improving the safety of patients: a national perspective

David Gerrett speaks about safety on a national scale
David Gerrett, senior pharmacist in the medication safety team at NHS England, takes to the stage.
If you get the right culture in a system it takes care of a lot of the issues we have got.
In 2004 we didn't really know what happened in primary care, we are starting that journey now.
From the NHS England perspective it's a good thing that you hold the reins on this and you develop it for yourself but it is the local learning that is the design of the NHS. It's not national top-down policy making any more.
It's important we realise as we change we can introduce inadvertently errors in structures and systems. It can become a worse system.
So we need to remember as things change in community pharmacy you have got to have something that is tracking this and I'm pleased to say through the MSO network you have this.
One billion prescriptions are issued every year in primary care. Don't feel that we don't appreciate that the system is already pretty good.
The reality is people at the cutting edge don't really understand the nature of errors - the vast majority are slips and lapses. Intentional errors are very rare.
But as the expectations of HCPs grows you may push people into situations where they are reckless.
If there's one message you need to make sure people understand the trap of feeling that being automated is a safe place to be - it's not.
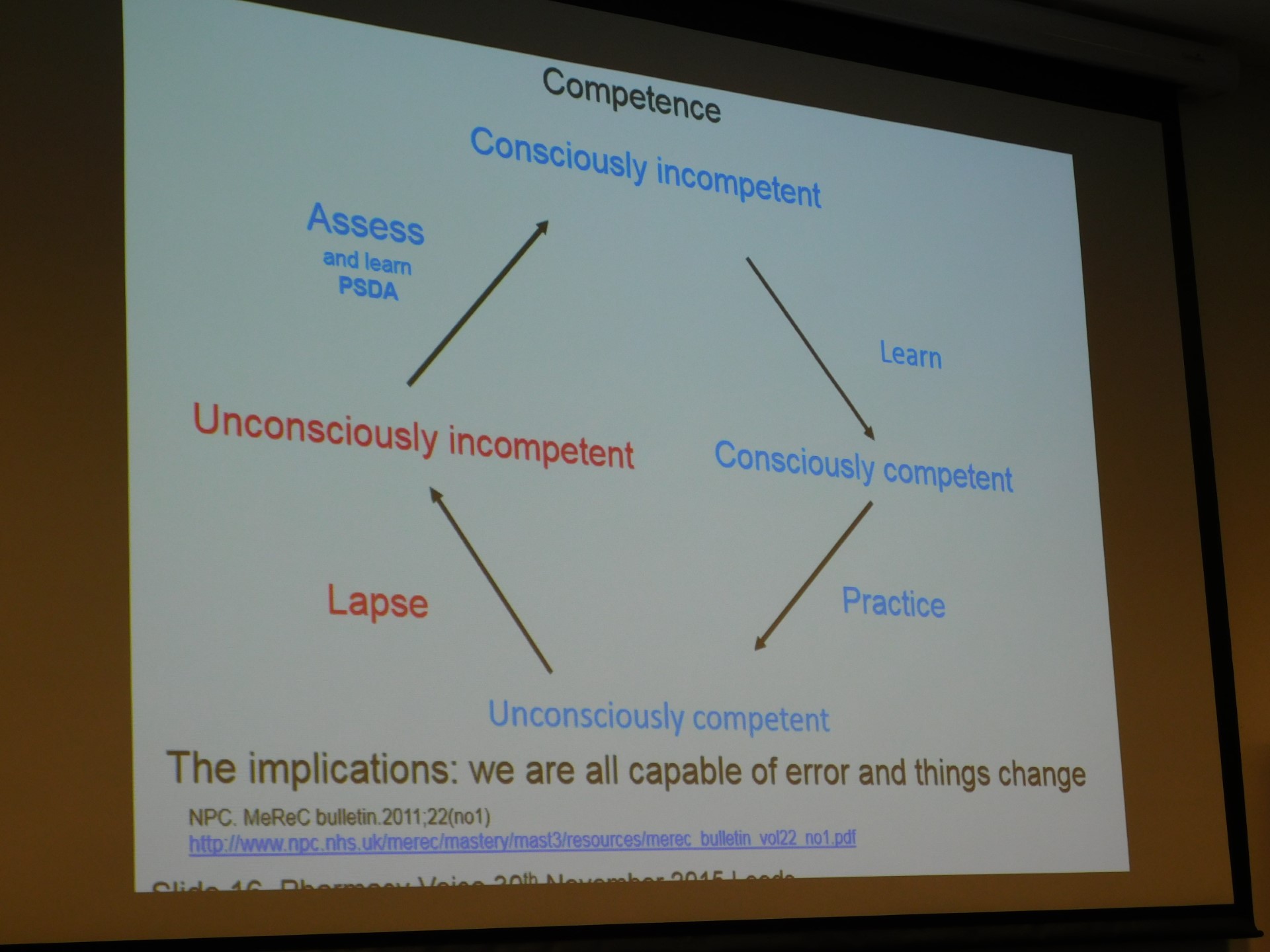
Cycle showing safety lapse
Medicines optimisation looks beyond the cost of medicines to the value they deliver and recognises medicines as investment in patient outcomes.
We are driving and giving you the steering wheel because the numbers of medication errors is very high.
The current buzzword is the Right Care programme - you need to look into this.
The big thing here is that everybody's communicating.
The MSOs in community pharmacy have had a lot of achievements - I think you can pat yourselves on the back because this is that start of a good journey. But you have to tell people about it - write it up, send reports to NHS England.
I think Pharmacy Voice is starting to do that.
10:30am: Is no-blame culture possible in healthcare? Lessons from the aviation industry

Aviation expert Carey Edwards draws parallels with pharmacy
Aeronautical safety expert and managing director of LMQ ltd, Carey Edwards, takes to the stage.
When I looked to find parallels between the industries I noticed we tend to try to kill people by the hundreds whereas you do them one-by-one.
But after looking at live maps of aircrafts I thought there is a lot of opportunity on an hourly basis within the aviation industry to make mistakes which could cause harm to a lot of people.
When we are concentrating on something else, we focus on what is going on there and we risk completely missing something else.
So we can miss seeing, hearing and feeling things.
There are one billion prescriptions a year - but it just needs one at the critical time.
The pressures we put people under - if they are thinking about other pressures they have - they may not be concentrating on the job in hand.
What happens is normally everything is going fine and suddenly it all goes downhill.
One wrong prescription out of a billion could cause a fatality - it's a big ask.
Human factors are anything that affects a person's performance.
There can be direct factors that affect performance. For example driving through a red light - you have either done it intentionally, it is as a result of dexterity problem, you are distracted or you lack awareness and don't notice it.
Then we have potential factors that make these more likely, including fatigue, memory, time, relationships, etc.
But what is important is the managing factors - training, performance reviews, checklists, motivating staff etc.
If we insist on a no-blame culture there will be issues with it. Firstly lazy people - people won't do anything, there will be a reluctance to update knowledge and skills and it will create resentment.
There is also an emotional need for someone to be punished and it is not acceptable to politicians, media and the public.
So there are big issues with a no-blame culture.
But there are also risks with a punitive culture - mistakes can be covered up, errors are not reported, people blame others and are reluctant to take risk. People are focused on abiding by rules rather than what is right for the patient.
The real question is which one on balance is better for long-term safety?
I think no-blame is better on balance because generally speaking we learn a lot more, people aren't generally lazy if recruited trained and motivated properly.
12:15pm: Sign up to safety and community pharmacy: three things you need to do differently now

Suzette Woodward explains how to do things differently
Suzette Woodward, national campaign director for NHS Sign up to Safety, takes to the stage.
Sign up to Safety is a national campaign, all you need to do is go to the website and pledge. It means you join a community of over 315 NHS organisations already.
It's not a top-down intervention, what it does is guide you to find the right things to make care safer. We look to help locally owned and self directed self-improvement.
Nurture a just culture in your pharmacy - it's both fairness and kindness when things go wrong but also accountability and responsibility.
"The single greatest impediment to error prevention is that we punish people for making mistakes" Dr Lucian Leape.
The best people can make the worst mistakes, systems will never be perfect and human beings will never be perfect.
A just culture is one where people who make an error are cared for and supported and people who don't adhere to policies and procedures are asked before being judged.
But those who put people at risk by reckless behaviour are held accountable for their actions.
The emphasis is on collecting information on incidents more but we need to collect better. If you have repeated reports of the same kind of event it suggests a poor culture of learning.
But if you have decreased reporting rates of similar types of incidents does that mean people have given up reporting?
We think we should focus all out efforts on the things that get reported the most. For example falls - that tend to be without blame and can be focused on easily. Other things are more complex and hard to report.
What can be done differently?
Think about an intelligent reporting system, focus on incidents that provide surprising insights into your safety system. Use those incidents to identify an prioritise significant or new emerging risk areas.
Expect your reports to be inaccurate or incomplete - but don't chase data constantly.
Use the reports to trigger an investigation.
How about not using an incident report at all?
Everyone is working hard but often they feel isolated an alone. Everywhere I speak in the NHS I have people coming up to me and telling me how exhausted they are.
Them and us culture is a waste of time - we need to be working together. Making care safer is complex and way too often we think about the solution and don't think about the complexity it will take to implement it.
Safety conversations can help remedy this.
Safety huddles involve bringing people together from your team each day for 30 seconds up to 10 minutes. It's not a big deal and doesn't take up much of your day.
Briefing and debriefing is an outstanding tool. What can we learn from the day that we can share day by day? This works well for teams that don't work together often.
You could also use facilitated debriefing post incident. What you need is just to sit down with people and figure out why things happened and how can you work on solutions.
There are five common causal factors: information, communications, observations, design and relationships. They tend to be the key factors as to why errors occur.
The experts are around you and surrounding you - think about your colleagues and patients because they will have the answers.
1:45pm: How can community pharmacy improve incident reporting and learning?
Rose Marie Parr, chief pharmaceutical offices for Scotland spoke to the conference over the telephone after adverse weather prevented her from travelling.
The overview of the rebalancing is about medicines legislation and pharmacy legislation - it is quite complex and does take some time.
The law does need to change to allow pharmacy to become more patient focused, more patient safety focused and more clinical in the future. It is also looking to the future about supervision and clinical pharmacy.
Decriminalisation of pharmaceutical errors will improve patient safety.
Rob Darracott, chief executive of Pharmacy Voice, takes to the stage.
Medicines are not ordinary items of commerce, this is at the heart of the challenges we are looking at.
A Programme Board for Rebalancing Medicines Legislation and Pharmacy Legislation has been established to examine the scope of legislation and regulation. Their role is to advise ministers and devolved administrations and to oversee the implementation of policy outcomes.
The rebalance is more reliance on professional regulation and less recourse to the criminal law. I think pharmacists will know what a challenge that has been, often very much about the perception of incidents or errors.
The board's scope includes a review of dispensing errors legislation, review of pharmacy professionals, hospital pharmacy regulation and pharmacist supervision.
The legislation under consideration is the Medicines Act 1968 and the Human Medicines Regulation 2012 and pharmacy regulation and orders for Great Britain and Northern Ireland.
Panel debate
- Celia Davies, patient representative
- Ash Soni, president of the Royal Pharmaceutical Society
- Leyla Hannbeck, chief pharmacist of the National Pharmacy Association
Q: What challenges do we have in engaging the public as we talk about doing things differently? How might we engage patients and the public?
CD: When I spoke to people their view at first was that decriminalising was really surprising, as though it was a backwards step. But after listening to some of the detail they would realise we would do much more about error reporting and improvement.
I think one part of the answer is not to talk about the public or the patient and start talking about different groups - designing something for the people using particular drugs. Working with older people I am horrified each time I see the statistics about medication adherence - it's going horribly wrong.
There's another stage, a bigger concept of error and involving people.
AS: We have got the consultation out now on professional standards on error reporting because for me, from a professional point of view, it's about not doing this in isolation.
If we empower pharmacists to be able to support their teams to be able to do the job more effectively and if we recognise that we are human and use that to get better that's a key part of the message we need to give from the profession as a whole. We need to move away from the principle of blame to the principle of learning.
We need to use that to make sure we don't repeat the same errors multiple times.
CD: But it's also about a better outcome and service improvement.
Q: What's the challenge for the NPA in the MSO role?
LH: We set up a survey together with NHS England about error reporting. Every month we are seeing increases in the level of reporting and it's great to see so many people taking the time to report and encouraging staff to do it as well.
Q: We seem to have focused on what we do when we do the wrong thing but what are the panel's views on the harm caused by omission?
AS: I think there is something around that that we need to do and it doesn't fit within this framework of legislation but it does with our responsibility to do the right thing at the right time. I think we also need to get the message to patients that they are entitled to things and can ask for it.
CD: Let's have a new and old medicines service. There are clearly political issues around things like this that need to be addressed.
LH: We need to link things together so people understand their relevance.
Q: Monitored dosage systems are the bane of every community pharmacy in the UK. It's unsafe and the patients devolve responsibility from administration from themselves to the pharmacist. How would the patients feel if community pharmacy refused to process monitored dosage systems and secondly do you agree with the devolvement of responsibility from patients or their carers to the pharmacist?
CD: We need, as the health service disintegrates around us, to recognise volunteers will need to become involved. But why not ask the patients?
Q: Job titles - I am a MSO and a superintendent pharmacist, we have a chief pharmacist on the stage. Are their too many titles? Do the public understand who is responsible?
AS: The challenge is not what the public understand, they care about the service we provide. I think the question is how do we defines roles themselves. That's one of the things about the Rebalancing Board is how do we become clear about what we are meant to do, when and how.
LH: To patients pharmacists are pharmacists, as long as we are clear in the profession who is accountable for what ultimately we are all accountable for patient safety.
CD: The most important thing is the person I meet when I walk into the pharmacy.

Have your say
Please add your comment in the box below. You can include links, but HTML is not permitted. Please note that comments are not moderated before publication and the views expressed are those of the user and do not reflect the views of The Pharmacist. Remember that submission of comments is governed by our Terms and Conditions. You can also read our full guidelines on article comments here – but please be aware that you are legally liable for any libellous or offensive comments that you make. If you have a complaint about a comment or are concerned that a comment breaches our terms and conditions, please use the ‘Report this comment’ function to alert our web team.